
New here? Start with the basics and where CAR-T is used today.→ A0: What Is CAR-T Therapy? The Big Picture + Series Index→ A1: Where CAR-T Is Used Tod
New here? Start with the basics and where CAR-T is used today.
→ A0: What Is CAR-T Therapy? The Big Picture + Series Index
→ A1: Where CAR-T Is Used Today — Blood Cancers First
What you will learn
- The short answer: CAR-T side effects are anticipated—and managed
- Think in three time windows (a simple mental model)
- Key side effect #1: inflammatory reactions (CRS) in plain language
- Key side effect #2: neurologic symptoms (ICANS) from a family perspective
- Recovery phase priorities: infection and low blood counts (cytopenias)
Want the deep dive (B2)? We will cover severity grading concepts, management tools, site operations, long-term follow-up, and regulatory logic.
→ B2: Toxicity management, site operations, long-term safety & regulatory logic [Expert]
The short answer: CAR-T side effects are anticipated—and managed
CAR-T therapy can trigger strong immune activation, so side effects can occur. The key idea is not “fear,” but preparedness: knowing what can happen, recognizing early warning signs, and contacting the care team promptly. Many terms (CRS, ICANS) sound intimidating; in this beginner post, we focus on the big picture and practical monitoring points.
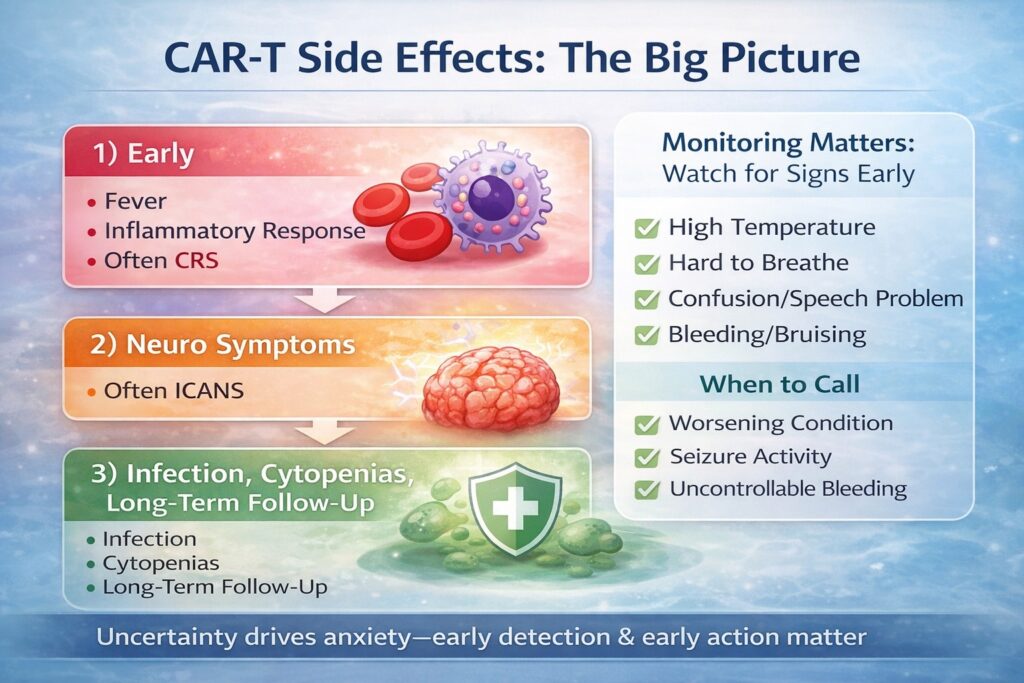
Think in three time windows (a simple mental model)
Side effects are easier to understand when grouped by “when they tend to show up.” Everyone is different, but this model helps patients and families plan.
1) Early: strong inflammatory reactions (often fever)
As CAR-T cells engage their targets, immune signaling can surge. This may appear as fever and systemic inflammation (often called CRS). For beginners, remember: fever can be an expected reaction, but it must be reported and managed early.
2) Early to mid: neurologic symptoms
Some patients experience temporary neurologic symptoms—confusion, difficulty speaking, unusual sleepiness, etc. Clinically this is often discussed as ICANS. The practical point is that monitoring matters, because early recognition can trigger timely interventions.
3) Recovery phase: infection risk, cytopenias, fatigue
Because many CAR-T regimens include pre-treatment (“conditioning”) and can affect blood counts, patients may have a period of low blood counts (cytopenias), increased infection risk, and prolonged fatigue. This is a major focus after discharge: what to watch for at home.
Key side effect #1: inflammatory reactions (CRS) in plain language
What can it look like?
- Fever (often the first signal)
- Chills, fatigue, poor appetite
- In some cases: low blood pressure, shortness of breath
Why does it happen?
When CAR-T cells activate, immune “messenger” molecules rise (cytokines). If the rise is strong, the body reacts with inflammation—often fever.
What patients/families should remember
- Fever is not automatically “danger,” but it is a reason to contact your team.
- Early reporting improves safety and keeps options open.
- Centers have established monitoring and management pathways.
Key side effect #2: neurologic symptoms (ICANS) from a family perspective
Possible signals
- Unusual confusion or disorientation
- Speech changes (word-finding difficulty, incoherent answers)
- Marked sleepiness or inability to focus
- Rarely: seizures
Why observation matters
Patients may not recognize subtle changes themselves. Family observations can be valuable when shared calmly and factually with the care team.
A safe way to help
- Ask short orientation questions (name, date, place) to detect changes.
- Report facts (what changed, when) without blaming or debating.
- When in doubt, contact the team early.
Recovery phase priorities: infection and low blood counts (cytopenias)
Why infection risk can rise
Pre-treatment and treatment effects can lower white blood cells temporarily. When defenses are down, infection risk increases—so fever after discharge matters.
Common warning signals
- Fever
- Cough, sore throat, shortness of breath
- Diarrhea, vomiting, severe fatigue
Practical prevention (not perfection)
- Hand hygiene; avoid crowded settings as advised; mask when appropriate.
- Food safety per your center’s guidance.
- Know the after-hours contact plan before discharge.
Other items worth knowing (so you don’t panic if you hear them)
Bleeding/bruising (platelet-related)
Low platelets can cause easy bruising or prolonged bleeding. Report concerning bleeding promptly.
Tumor lysis syndrome (TLS)
If therapy works rapidly and many tumor cells break down at once, body chemistry can shift. Teams watch and prevent this risk in higher tumor-burden settings.
Long-term follow-up
Immune recovery can take time. Your team may discuss vaccination timing and infection prevention plans. Track your recovery pace and share changes with your clinicians.
“When should we call?” Decide this early
Much anxiety comes from uncertainty about thresholds. Follow your center’s instructions, but in general, contact your team early for:
- Fever (especially after discharge)
- Breathing difficulty, severe dizziness, fainting
- Confusion, speech changes, seizure-like activity
- Uncontrolled bleeding, black stools, severe abdominal pain
- A strong sense that the patient is “getting worse”
Questions to ask your care team (copy/paste)
- Which side effects are most relevant for me, and when?
- What are your specific call thresholds (temperature, symptoms)?
- What is the after-hours contact plan?
- What infection precautions should we follow at home?
- How long do you expect low blood counts, and how often are labs checked?
FAQ
Q1. Do side effects happen to everyone?
No. Type and severity vary. Prepared monitoring reduces risk and helps the team act early if needed.
Q2. Does CRS/ICANS mean the treatment is working?
Not necessarily. Immune activation can correlate with response in some contexts, but it is not a simple “more is better” rule. Safety management comes first.
Q3. How long do we need to be vigilant after discharge?
The focus shifts over time: early fever/neuro monitoring transitions toward infection prevention, blood count recovery, and stamina rebuilding.
What’s next
Next is the expert post (B2), covering management concepts, site operations, long-term safety, and regulatory logic.
→ B2 [Expert]
Mini glossary
- CRS: inflammatory reaction associated with immune activation (often fever).
- ICANS: a category of neurologic symptoms that can occur after CAR-T.
- Cytopenias: low blood counts (white cells, red cells, platelets).
- TLS: metabolic shifts caused by rapid tumor breakdown.







Comments