
Prefer the beginner overview first?→ A0: What is CAR-T therapy? The big picture + index→ A2: CAR-T side effects without panic (what happens, what to m
Prefer the beginner overview first?
→ A0: What is CAR-T therapy? The big picture + index
→ A2: CAR-T side effects without panic (what happens, what to monitor)
What you will learn
- Executive summary
- 1) The operational coordinate system: what to watch, when, and how to escalate
- 2) CRS (cytokine release syndrome): practical monitoring and intervention logic
- 3) ICANS: turning family-observed changes into actionable clinical signals
- 4) Post-discharge operations: infection, prolonged cytopenias, and triage design
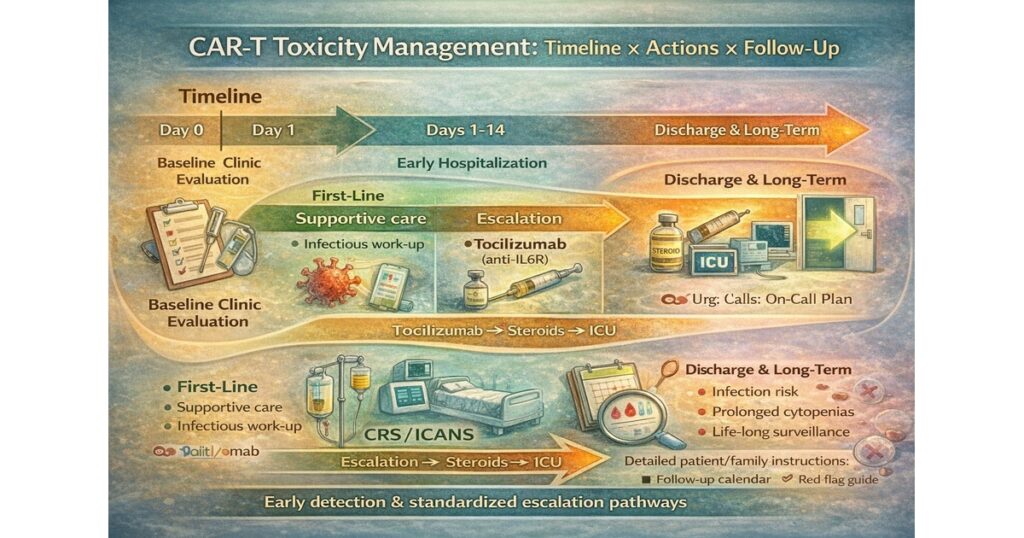
“CAR-T Toxicity Management: Timeline × Actions × Follow-Up”
Left: Day 0–14 (CRS/ICANS peak) | Middle: First-line→Escalation | Right: Discharge→Long-term | Bottom: early detection matters
Executive summary
- CAR-T toxicity management is not “endure severe side effects,” but a system of early detection → standardized escalation pathways to prevent progression.
- Most centers speak a common language using ASTCT consensus grading for CRS and ICANS, enabling rapid multi-team coordination.
- FDA eliminated REMS for currently approved BCMA- and CD19-directed autologous CAR-T immunotherapies (Jun 2025), reflecting mature risk communication via labeling/Medication Guides.
- In parallel, FDA required class labeling updates (boxed warning changes) highlighting T-cell malignancy risk (Apr 2024). In practice, this means simplified access + stricter long-term safety framing.
- Operational excellence is driven by triage, 24/7 escalation, drug availability, and protocol discipline, not by “never sending patients to ICU.”
1) The operational coordinate system: what to watch, when, and how to escalate
Time windows
- Early (often within ~2 weeks): CRS (fever, hypotension, hypoxia) and ICANS (confusion, aphasia, seizures) cluster here
- Recovery phase: infections, prolonged cytopenias, fatigue, readmission triggers
- Long term: secondary malignancy surveillance, immune reconstitution, revaccination planning
Why ASTCT grading matters
CRS and ICANS must be quantified consistently; ASTCT grading anchors escalation decisions. A key practical point: after antipyretics/anti-cytokine therapy, CRS grading is driven by hypotension/hypoxia, not fever.
2) CRS (cytokine release syndrome): practical monitoring and intervention logic
What teams “catch” first
- Fever, chills, malaise
- Progression markers: hypotension and hypoxia (these drive escalation)
The intervention skeleton (First-line → Escalation)
- First-line: supportive care + infectious work-up in parallel; early IL-6 pathway blockade (e.g., tocilizumab) per protocol
- Escalation: persistent/worsening hypotension/hypoxia → add corticosteroids and intensify monitoring/ICU coordination
The common pitfall: CRS vs infection
They overlap. The practical rule is to evaluate infection while not delaying CRS-directed management when clinically indicated.
3) ICANS: turning family-observed changes into actionable clinical signals
Typical presentations
- confusion, disorientation, word-finding difficulty/aphasia
- marked somnolence, inattention
- seizures (rare but critical)
ICE-style screening logic
ICANS can be tracked using structured bedside assessments (ICE concepts) to enable clear handoffs.
Management skeleton
- ICANS may not respond to IL-6 blockade alone; corticosteroids are central in many protocols
- seizure risk management with anti-seizure medications, and escalation to ICU/EEG/imaging as needed
4) Post-discharge operations: infection, prolonged cytopenias, and triage design
Key operational elements:
- 24/7 contact routing (who answers, who decides)
- explicit thresholds: temperature/symptom triggers for call/ED
- standardized prophylaxis and revaccination planning per center
- “one-page” patient/family instructions (highest ROI intervention)
5) Site operations after REMS elimination: what still matters
REMS elimination is not “risk is gone”; it’s “risk can be managed without REMS burden.”
Centers still need:
- trained teams + clear escalation ownership
- drug availability + rapid diagnostics
- written protocols + continuous improvement loops
6) Long-term safety: boxed warning logic and lifetime surveillance framing
FDA concluded T-cell malignancy risk applies across currently approved BCMA- and CD19-directed genetically modified autologous CAR-T products and required boxed warning changes.
Operational implications:
- long-term follow-up planning becomes non-optional
- patient counseling and documentation must match the labeling posture
- surveillance is a system, not a one-time warning
7) CMC/comparability: the foundation that can shift efficacy/toxicity at scale
FDA’s CAR-T guidance explicitly addresses CMC and analytical comparability for ex vivo CAR-T products.
For sponsors and evaluators, “comparability strategy” is a proxy for whether a program can scale without surprises.
Primary sources
FDA REMS elimination press release (Jun 2025).
FDA boxed warning on T-cell malignancies (Apr 2024).
FDA CAR-T development guidance (Mar 2024).
ASTCT CRS/ICANS consensus grading (2019).
Editors Note
This article covered the following key points:
- Executive summary
- 1) The operational coordinate system: what to watch, when, and how to escalate
- 2) CRS (cytokine release syndrome): practical monitoring and intervention logic
- 3) ICANS: turning family-observed changes into actionable clinical signals
Rather than fragmented news or definitions, the aim was to present these as a single connected flow. For one step deeper on the same theme, see the related articles below.







Comments