
Prefer the beginner overview first?→ A3: Why solid tumors are hard for CAR-T (the 3 barriers)
Prefer the beginner overview first?
→ A3: Why solid tumors are hard for CAR-T (the 3 barriers)
What you will learn
- Executive summary
- 1) The core framework: 3 barriers × 3 engineering levers
- 2) Solving Barrier 3: multi-target and logic-gated CARs
- 3) Solving Barrier 2: armoring, inhibitory-signal resistance, and rewiring exhaustion
- 4) Solving Barrier 1: access redesign (locoregional delivery + “make them home”)
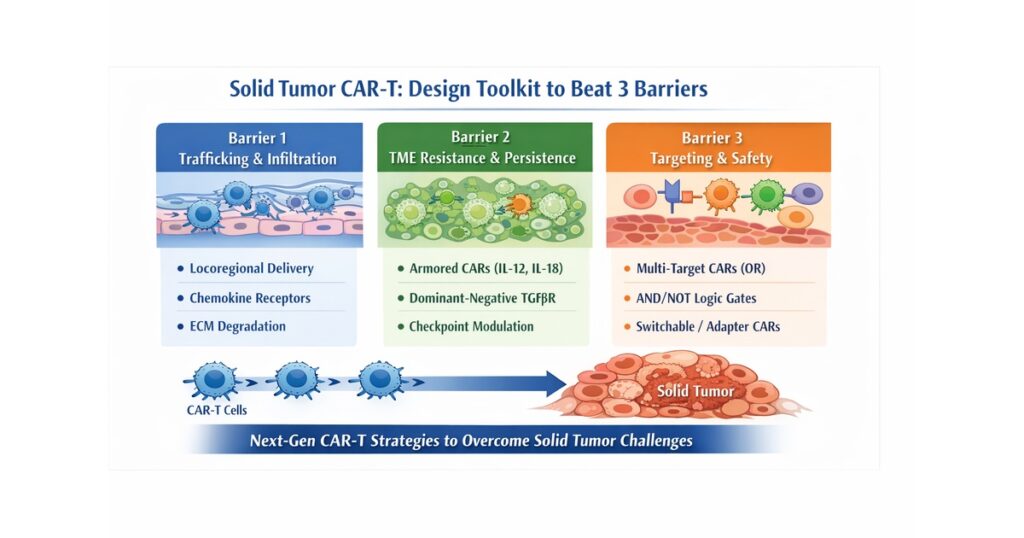
“Solid-Tumor CAR-T Design Toolkit to Beat 3 Barriers” (Trafficking / TME resistance / Target & safety)
Executive summary
Solid-tumor CAR-T is not failing for mysterious reasons—it is hard for well-defined ones. The field is converging on a clear engineering thesis:
- Targeting + safety redesign (multi-target OR gates, AND/NOT logic, controllable adaptor CARs)
- TME resistance + persistence (armored CARs, dominant-negative/switch receptors, checkpoint rewiring)
- Access redesign (locoregional delivery, trafficking and infiltration engineering)
Clinically, locoregional delivery—especially in CNS tumors—has produced feasible safety profiles and signals of activity in subsets, shifting the narrative away from “solid tumors are impossible.”
1) The core framework: 3 barriers × 3 engineering levers
Barrier 1: trafficking/infiltration
- Lever A: locoregional delivery
- Lever B: enhanced homing (chemokine-receptor matching)
- Lever C: enhanced penetration (ECM/stromal barriers)
Barrier 2: TME suppression/exhaustion
- Lever A: armoring (TRUCK)
- Lever B: resistance to inhibitory signals (dominant-negative/switch receptors)
- Lever C: persistence/fitness engineering
Barrier 3: target heterogeneity + safety
- Lever A: OR logic (multi-target)
- Lever B: AND/NOT logic (logic gating)
- Lever C: adaptor/switchable CARs (controllability)
This taxonomy is now widely reflected across solid-tumor CAR reviews.
2) Solving Barrier 3: multi-target and logic-gated CARs
OR gates: reduce antigen escape
Multi-target CARs (tandem/bicistronic) aim to recognize either antigen, improving robustness against heterogeneous tumors—at the cost of potentially broader normal-tissue recognition.
AND gates: raise specificity and safety
Logic-gated designs (e.g., synNotch-type strategies, split receptors) require two conditions to trigger full killing, addressing the “no perfect target” reality in solid tumors.
NOT gates: avoid healthy tissue
Inhibitory CAR concepts use a “healthy-tissue antigen” to brake activation, aiming to reduce on-target/off-tumor toxicity.
Adaptor (universal) CARs: dose-controlled, target-swappable
Adaptor systems decouple the CAR from the tumor antigen, enabling controllability (on/off) and retargeting—highly attractive operationally for solid tumors.
3) Solving Barrier 2: armoring, inhibitory-signal resistance, and rewiring exhaustion
Armored CARs / TRUCK
Cytokine engineering (e.g., IL-12/IL-18 concepts) aims to reshape the TME locally and sustain function.
Dominant-negative / switch receptors (TGF-β axis as a canonical example)
TGF-β is a major suppressive pathway in many solid tumors; dominant-negative receptor strategies are repeatedly highlighted as a rational countermeasure.
Checkpoint rewiring
PD-1 axis editing/reprogramming is actively explored, but must be evaluated carefully for safety and durability trade-offs.
4) Solving Barrier 1: access redesign (locoregional delivery + “make them home”)
Locoregional delivery: CNS tumors as a proving ground
Locoregional IL-13Rα2 CAR-T delivery in recurrent high-grade glioma has reported feasibility and promising activity in subsets.
Homing engineering
Chemokine-receptor matching seeks to pull CAR cells into tumors; evaluators should look for direct evidence of tumor localization.
Penetration engineering
Strategies to overcome ECM/stromal barriers are conceptually strong but must balance local inflammation and safety.
5) Solid-tumor antigen patterns worth recognizing (representative set)
In CNS solid-tumor CAR literature, repeatedly discussed antigens include IL13Rα2, HER2, EGFR/EGFRvIII, EphA2, GD2, B7-H3, among others.
6) Beyond autologous T cells: allogeneic CAR and CAR-NK
Allogeneic CAR approaches are increasingly reviewed as ways to improve turnaround time, cost, and access.
CAR-NK is frequently framed as a potentially safer, off-the-shelf alternative, though persistence/infiltration/TME resistance remain key hurdles.
7) What to watch in the next 12–24 months (catalysts)
- Reproducibility of locoregional CNS CAR activity signals
- First meaningful clinical readouts for logic-gated / multi-target CARs
- Whether armoring / inhibitory-signal resistance improves durability without unacceptable toxicity
- Operational maturation of allogeneic / CAR-NK platforms
Editors Note
This article covered the following key points:
- Executive summary
- 1) The core framework: 3 barriers × 3 engineering levers
- 2) Solving Barrier 3: multi-target and logic-gated CARs
- 3) Solving Barrier 2: armoring, inhibitory-signal resistance, and rewiring exhaustion
Rather than fragmented news or definitions, the aim was to present these as a single connected flow. For one step deeper on the same theme, see the related articles below.
Key references
Solid-tumor CAR design overviews and “toolkit” framing
Locoregional IL-13Rα2 CAR-T in recurrent high-grade glioma
Allogeneic CAR and CAR-NK clinical trend reviews







Comments