CAR-T therapy is one of the cancer treatments that has attracted particularly strong expectations in recent years. In fact, in relapsed or refractory hematologic malignancies, it can produce deep responses that were difficult to achieve with conventional therapies, and for some patients and families it is often described as a “last resort.”
At the same time, as we discussed in A5 and B5, the world of CAR-T is now expanding beyond ex vivo approaches, in which cells are engineered outside the body, toward in vivo approaches, in which CAR cells are generated inside the body itself. From 2025 into 2026, major pharmaceutical companies moved aggressively into in vivo CAR-T, including AbbVie’s acquisition of Capstan, Kite’s acquisition of Interius, and Eli Lilly’s acquisition of Orna Therapeutics in February 2026. Lilly specifically highlighted Orna’s in vivo CAR-T pipeline, especially its CD19-directed autoimmune programs, and stated that the total deal value could reach up to $2.4 billion including milestones. This wave of transactions suggests that in vivo CAR-T is no longer viewed as merely an exciting scientific concept, but increasingly as a platform that may help address the long-standing barriers of cost, manufacturing, and patient access. (investor.lilly.com)
However, one point is essential: a treatment receiving attention and a treatment truly reaching patients at scale are not the same thing.
Even if CAR-T is highly promising, there are many hurdles before a patient can actually receive it. It is expensive. Only limited centers can administer it. Manufacturing takes time. And some patients’ disease may progress too quickly to wait for that manufacturing window. These factors overlap to create situations in which a therapy is “available in theory” but “not accessible in reality.” In this article, we will organize that reality of price and access as clearly as possible. (nature.com)
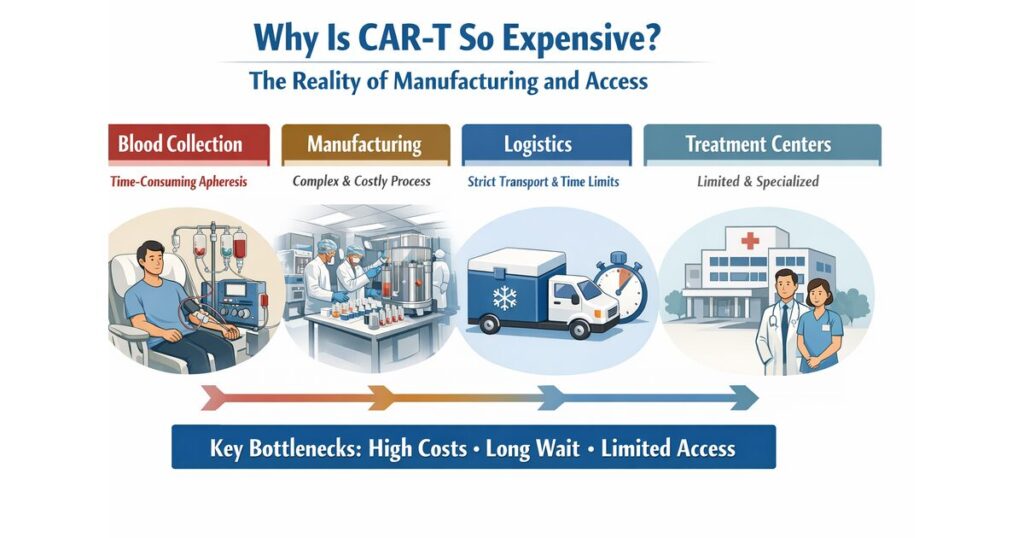
Why Is CAR-T So Expensive?
The short answer is that CAR-T is expensive not simply because it is “innovative.”
It is expensive because it is, in many cases, an almost individualized medical product manufactured separately for each patient.
Most conventional pills or antibody drugs are mass-produced in factories, and the same product can be used for many patients. By contrast, many autologous CAR-T therapies start with collecting T cells from the patient, genetically engineering them, expanding them, performing quality testing, and then sending them back to the hospital. In other words, CAR-T is both a product and a living, personalized therapy made from the patient’s own cells.
That alone makes its cost structure fundamentally different from that of ordinary pharmaceuticals. (nature.com)
Moreover, the total cost is not determined only by “making the cells.” At a minimum, several major cost layers are involved.
1. The Cost of Cell Collection and Preparation
The first step is collecting T cells from the patient.
This is not a simple blood draw. It is usually done through a specialized procedure called apheresis. Depending on the patient’s condition, blood counts, and prior treatments, collecting enough functional cells may itself be difficult. So from the very beginning, specialized equipment and trained personnel are already required.
2. The Cost of Genetic Engineering and Cell Expansion
The central step of CAR-T manufacturing is introducing the CAR gene into the collected T cells and expanding them.
This requires expensive materials such as viral vectors, controlled sterile environments, and highly skilled operators. In addition, each patient’s product must be managed as a separate lot, which means the efficiency of typical mass production is much harder to achieve. Because manufacturing conditions and quality variation can directly affect clinical performance, CAR-T production is intrinsically complex and costly. (nature.com)
3. The Cost of Quality Testing
Once the cells are made, they cannot simply be used immediately.
They must pass multiple quality tests, including checks for cell number, activity, sterility, and whether the intended genetic modification has been introduced properly. Compared with chemically synthesized drugs, living cell products are much harder to standardize, and the burden of quality assurance is significantly higher. (nature.com)
4. The Cost of Logistics and Time Control
For many CAR-T products, the collected cells must be sent to a manufacturing site and the final product then returned to the treating hospital.
This round trip requires strict temperature control and precise chain-of-identity and chain-of-custody management. Even minor errors are unacceptable. Because the product is derived from the patient’s own cells, a mix-up must never happen. As a result, logistics in CAR-T are far more demanding than in standard pharmaceuticals.
This “invisible but very expensive logistics layer” is one of the major forces driving up CAR-T pricing. (nature.com)
5. The Cost of the Hospital Delivery System
CAR-T does not end with purchasing a product.
The treating center must have systems for patient selection, lymphodepleting preconditioning, acute toxicity monitoring, ICU collaboration, and long-term follow-up. In particular, experience with managing CRS and ICANS is critical, meaning CAR-T is not a therapy that can be delivered safely anywhere by anyone. As we discussed in B2, CAR-T depends not only on “drug cost,” but also on the existence of a hospital system capable of operating it safely. (nature.com)
Where Do Patients Get Stuck?
The barrier to CAR-T is not price alone.
From the patient’s point of view, the deeper problem is often time and reachability.
1. Having an Indication Does Not Mean You Can Actually Receive It
Even if a patient fits the formal indication for CAR-T, not everyone can ultimately receive it.
Disease may be progressing too fast. There may be active infection. The patient’s overall condition may be too poor. Referral may come too late. Or the treating center may not have capacity. Because of these real-world factors, some patients who are technically eligible never make it to treatment. In CAR-T, vein-to-vein time—the interval from cell collection to reinfusion—is recognized as a clinically important issue. (nature.com)
2. The Disease May Progress While Waiting for Manufacturing
In autologous CAR-T, there is an unavoidable waiting period between cell collection and product return.
During this time, bridging therapy may be needed to control the disease. But not every patient can safely wait through that interval.
Even if CAR-T is “an effective therapy,” it loses meaning if the disease advances before the treatment can arrive. This is one of the most serious barriers from the patient’s perspective. (nature.com)
3. Treatment Centers Are Limited
Because CAR-T requires specialized systems, it cannot be delivered at every hospital.
That creates regional and institutional disparities. Some patients may need to travel long distances or remain near a treatment center for extended periods. This creates not only physical and psychological burdens, but also practical strain on families, work, and daily life. In resource-limited settings, reimbursement, regulation, infrastructure, and staffing all combine to become barriers to implementation. (ashpublications.org)
4. Treatment Does Not End at Infusion
CAR-T is not something that ends once the cells are infused.
In addition to monitoring acute toxicities, clinicians must also watch for infections, hypogammaglobulinemia, and long-term safety issues. In other words, what patients need is not simply one infusion, but an entire continuum of care before and after treatment.
Without understanding that, it is hard to fully appreciate why CAR-T is such a large and complex undertaking. (nature.com)
Why CAR-T Is Still So Special
At this point, CAR-T may sound like an extremely difficult and expensive therapy.
Yet it continues to be pursued worldwide because when it works, the impact can be extraordinary.
Most drugs need to be taken continuously or given repeatedly to suppress disease.
CAR-T, by contrast, gives the patient’s own immune cells a new function, turning them into a kind of “living therapy” that can seek out and attack the target inside the body.
It is certainly not a universal cure, but because some patients achieve deep remissions and long-lasting benefit, the field continues to move forward. (nature.com)
Moreover, the field is now expanding beyond cancer into autoimmune disease.
The reason companies like Orna and Capstan are being taken seriously by major pharma players in autoimmune settings is that CAR-T may evolve from being “an ultra-complex therapy for a limited subset of cancer patients” into a broader form of immune-reset medicine that could reach much larger patient populations. (investor.lilly.com)
What Is In Vivo CAR-T Trying to Change?
The in vivo CAR-T approaches we discussed in A5 and B5 connect directly to the theme of this article.
The reason this technology is drawing so much attention is that it may be able to change the core bottlenecks in manufacturing and access.
With conventional autologous CAR-T, cells must be collected from each patient, manufactured outside the body, and then shipped back.
With in vivo CAR-T, the goal is to deliver the genetic information or program directly into the body and generate CAR-expressing immune cells in vivo. If this works as intended, it could reduce or bypass parts of apheresis, individualized manufacturing, and complex logistics.
In other words, it could move the field toward something faster, more scalable, and potentially deliverable at more centers. (investor.lilly.com)
This area is already moving beyond pure concept.
Interius announced first-patient dosing with its in vivo CAR gene therapy and later reported expansion of clinical permissions in Europe. Umoja received FDA Fast Track designation for its in vivo CAR-T candidate for CD19-positive B-cell malignancies and had previously announced IND clearance in 2024. In addition, a Nature Medicine paper published on March 25, 2026 reported a phase 1 study of anti-BCMA in vivo CAR-T in five patients with relapsed or refractory multiple myeloma, with objective responses in 4 of 5 patients and stringent complete remission in 3 of them. The cohort is very small and follow-up remains limited, so broad conclusions would be premature. Still, it is increasingly clear that the idea of “generating CAR-T inside the body” is beginning to look clinically real. (interiusbio.com)
That said, in vivo CAR-T will not solve everything overnight.
Which cells in the body receive the program? At what level? For how long? Can off-target cell types be avoided? Can expression be controlled tightly enough? How will CRS and neurotoxicity be managed? And how should CMC and regulatory thinking be redesigned?
As we explored in B5, reducing the complexity of factory manufacturing does not remove complexity altogether. It shifts the hardest questions toward in vivo delivery, expression control, and safety design. For that reason, it is most realistic to think that conventional CAR-T and next-generation CAR-T platforms will coexist for some time. (nature.com)
Allogeneic CAR-T Is Another Important Candidate for Improving Access
Another important strategy for improving access is allogeneic CAR-T.
This refers to “off-the-shelf-like” approaches in which cells are prepared in advance from healthy donor material or similar sources, rather than manufactured individually from each patient.
Compared with autologous CAR-T, this model may offer faster availability and greater manufacturing standardization.
Of course, it comes with its own challenges, including rejection, GVHD, and persistence. But in terms of reducing the burden of patient-by-patient production, it points in the same direction as in vivo CAR-T.
In other words, one of the central themes of next-generation CAR-T is not only whether it can work, but whether it can reach patients in time and at scale. (nature.com)
What Needs to Happen for Prices to Come Down?
To lower the price of CAR-T in a meaningful way, simple price negotiation is not enough.
The underlying structure itself has to change.
1. Standardization of Manufacturing
If the manufacturing process becomes more reproducible and lot-to-lot variability decreases, failure rates and the need for remanufacturing can be reduced.
That ultimately supports lower costs.
2. Greater Efficiency in Materials, Vectors, and Quality Testing
Expensive raw materials and complex testing systems are major drivers of current CAR-T cost.
If these can be improved, the economic foundation of CAR-T will change.
3. Expansion of Treating Centers
If delivery can be expanded beyond a handful of ultra-specialized centers to a broader group of hospitals that meet defined requirements, patient access will improve.
But this must not come at the expense of safety, so training, referral networks, and remote support systems all matter.
4. Reimbursement and Real-World Implementation Design
For high-cost therapies like CAR-T, science alone is not enough; payment systems matter too.
Rather than stopping at “it is too expensive to use,” healthcare systems need to clarify in which patient groups CAR-T creates the most value and at what point in treatment it should be used. In the long run, that is part of how access improves. (ashpublications.org)
What Truly Matters for Patients and Families
From the patient and family perspective, the most important thing is not to see CAR-T as either a “miracle therapy” or simply “a treatment that is too expensive.”
In reality, CAR-T is a therapy with significant potential, but one that only works when preparation, waiting time, toxicity management, and treatment-center systems all come together.
That is why discussions with the treating team need to focus on practical questions.
Is the patient truly eligible now? Should referral happen urgently? Can the disease be controlled during the waiting period? Is there an accessible center nearby? What kind of family support will be needed?
With CAR-T, the key is not only “whether to receive it,” but also whether the opportunity to receive it can be lost before it is reached. (nature.com)
Conclusion: The Next Battle for CAR-T Is Shifting from “Can It Work?” to “Can It Reach Patients?”
CAR-T has already changed the future of cancer therapy.
But the next battle is no longer just about response rates.
What will matter from here is:
How quickly can the therapy reach patients?
How safely can it be delivered across more treatment centers?
How can it be supported by pricing and reimbursement systems that society can sustain?
In that sense, recent moves such as Orna × Eli Lilly, Capstan × AbbVie, Interius × Kite, Umoja’s progress, and the first clinical reports of in vivo CAR-T all point in the same direction.
The future of CAR-T is not only about making stronger cells. It is about breaking through the barriers of manufacturing, logistics, and access. (investor.lilly.com)
The in vivo CAR-T approaches we covered in A5 and B5 are among the strongest candidates to help answer that challenge.
But they are not magic.
In reality, conventional CAR-T, allogeneic CAR-T, and in vivo CAR-T will likely continue to advance in parallel, each with its own strengths and weaknesses, until the field gradually converges on approaches that are truly timely and reachable for patients.
The real future of CAR-T will not be decided only in the laboratory.
It will also be decided in hospitals, in logistics systems, in regulatory frameworks, in reimbursement design, and in the practical treatment journey of each patient.
So if there is one core message to remember from A6, it is this:
The central challenge of CAR-T is not only whether it works, but whether it can reach patients in time.
And right now, the world is beginning to attack that barrier in earnest. (nature.com)
Comments